The aortic valve is the exit point for blood being pumped to the rest of the body, regulating the single-directional flow of blood out of the heart. If the valve cannot open completely (aortic stenosis), the heart is forced to pump harder against the narrowed opening. Conversely, if the aortic valve does not close completely (aortic regurgitation or insufficiency), blood leaks back into the heart, similarly forcing the organ to work harder. Both pathologies will eventually lead to heart failure and reduced life expectancy, if left untreated. The most common causes of aortic valve disease include congenital disorders, rheumatic valvular disease or calcification of adulthood. Patients can have an asymptomatic period before developing symptoms such as fainting, tiredness, shortness of breath and/or chest pains.
For more information about aortic stenosis, please click here.
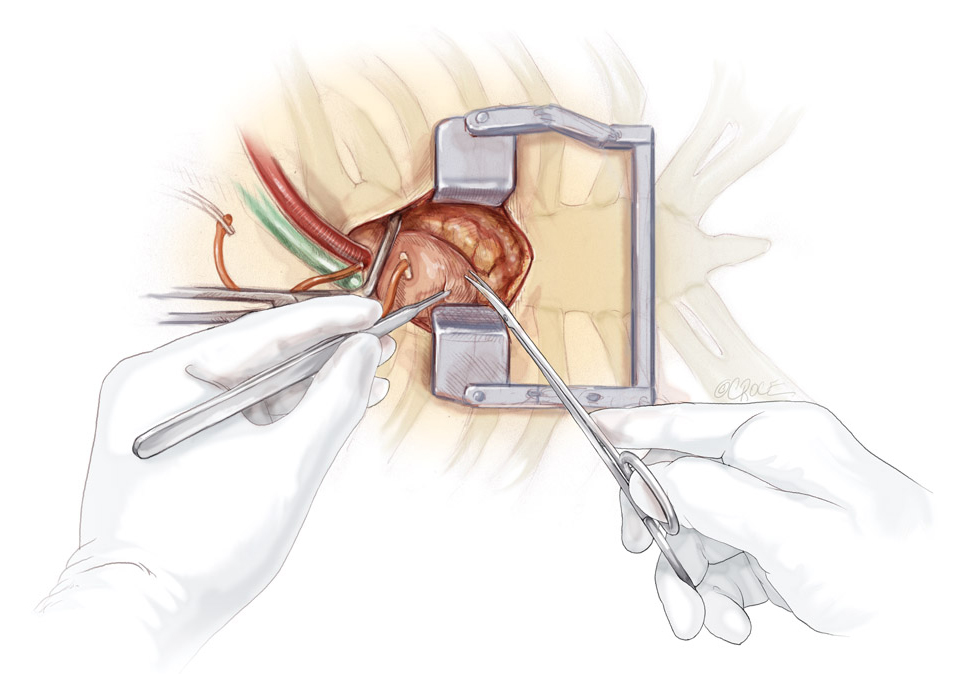
Surgical Options
When the aortic valve is too diseased, surgical replacement is necessary to reduce symptoms and improve life expectancy. The specific choice of valve (for example, an tissue valve or a mechanical valve) is am important issue and dependent on the patient's age and preference. The traditional surgical approach requires a 20 cm opening in the middle to access the heart (median sternotomy) and the use of a cardiopulmonary bypass machine, which acts as the heart and lungs to support the patient’s body when the heart is stopped. A minimally invasive approach has the benefits of faster recovery and better cosmesis.
Mini-sternotomy approach: a small 5-8 cm (2-3 inch) long cut is made along the upper part of the sternum only. All surgical steps are made through this smaller incision using long and refined instruments. Heart and lung machine is employed routinely. The potential benefits include less blood loss, better cosmsis and faster recovery.
Mini-thoracotomy approach: a small 5-8 cm (2-3 inch) long cut is made on the right side of the chest below the collar bone. Through this a small cut, an access to the the heart is achieved. However, in this approach a rib is divided and usually a small cut in the groin is required to established cardiopulmonary bypass.
Our recent study has shown similar results between these two minimally invasive approaches, but both techniques have the following advantages over the traditional open chest operation:
Reduced blood loss
Reduced risk of sternal complications
Faster recovery and shorter hospital stay
Less scarring and better cosmetic appearance
Suitability
The suitability for minimally invasive aortic valve replacement is assessed on an individual basis. Approximately 85-90% of patients are suitable for a minimally access approach. Often it depends on the heart function, chest anatomy and co-existing medical conditions. Another important issue that needs to be considered is whether a mechanical or a tissue valve is more suitable to you. A mechanical valve is very durable, but it requires you to take a blood-thinning medication, warfarin, for the rest of your life. A tissue valve may only last for 7-15 years, but does not require warfarin. Professor Tristan Yan will discuss the safest and most appropriate option with you at the time of your consultation. For more information, please click here.